
Research Article | DOI: https://doi.org/10.31579/2641-8975/009
*Corresponding Author: Paul Aveyard, University of Pittsburgh Diabetes Institute, UK.
Citation: Paul Aveyard and Jean-Francois Etter, The A1c and blood glucose levels of the diabetic patients in the EG were lower of than those of the individuals in the CG, DOI:10.31579/2641-8975/009
Copyright: © 2018 Paul Aveyard.et.al.This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 June 2018 | Accepted: 14 June 2018 | Published: 22 June 2018
Keywords: Diabetes mellitus, Glycemic control, Videophone, Telecare
Background: Prevention of diabetic complications requires good glycaemic control. This study aimed to provide type 2 diabetes patients with remote active care and glycaemic control through the use of videophone technology without the need for them to attend hospital. The literature recommends additional research to study the impact of technical innovations on improved disease self-management and medical outcome. This is the only study to be conducted in Turkey concerning patient monitoring using videophone technology. The aim of the study was to establish the effectiveness of the use of videophone technology in the glycaemic control of patients with diabetes living in remote areas.
Methods: This is a prospective, randomized control study using the systematic sampling method (using half ratio), in which 24 patients were chosen for the Experimental Group (EG) and another 24 for the Control Group (CG). All of the patients agreed to participate in the study. Patients in the CG received routine care, while the glycaemic control and consultations for patients in the EG were conducted using videophone technology. The patients were monitored by videophone for a total of 6 months. The HbA1c and blood glucose values recorded over the 6 month monitoring period were analyzed to determine the effectiveness of using a videophone.
Results: The mean age of the individuals in the EG was 54.41 ± 8.54 years (Min=43 Max=78) and in the CG it was 57.25 ± 9.61 (Min=40 Max=77). In both groups, 50% of the individuals were men and 50% were women. When the two groups were compared, it was was found that the preprandial blood glucose levels of the diabetic patients in the EG (mean 159.48 ± 40.71mg/dl) were lower by 13.55 ± 52.89 mg / dl than the preprandial blood glucose levels of the diabetic patients in the CG (mean 173.03 ± 65.07 mg/dl). It was determined at the end of the six-month monitoring that the A1c levels of the individuals in the EG were significinatly lowered by 0.49% in total, and that the A1c levels of the individuals in the CG were higher by 0.17 % in total.
Conclusions: It was shown that videophone technology can be useful in the glycaemic control of diabetic patients in Turkey.
Diabetes is a leading cause of death and morbidity and is a health priority worldwide. An estimated 285 million people worldwide have diabetes and its prevalence is predicted to increase to 439 million by 2030 [1].
Diabetes is one of the most important non-communicable diseases in Turkeycountry and constitutes a disease burden which is expected to rise even further in the near future [2,3]. In the Turkish Diabetes Epidemiology Study (TURDEP) by Satman et al., the prevalence of diabetes mellitus in Turkey was established as 13.7% and the prevalence of impaired glucose tolerance was 14.5%. The rate of diabetes mellitus and impaired glucose tolerance was also shown to rise along with increases in BMI, waist/ hip ratio and waist circumference [4].
The increase in the use of technology in diabetes treatment facilitates improved communication between nurses and patients, the reliable collection of data, and the provision of a comfortable life to patients [5,6,7,8]. Another important purpose of tele-care is to provide patients with the opportunity to maintain their education effectively without interruptions [9,10,11]. Videophone technology, using webcams and with regular telephone consultations, enables patients to maintain their education, and to have treatment at home without the need to attend clinics. Through the use of technical instruments such as videophones, the needs of patients with different metabolic control needs can be met [12].
Videophone technology allows possibilities such as easy face-to-face communication between diabetes patients and health professionals, the self-monitoring of blood glucose levels and receiving feedback (support and counselling) [13,14]. This technology, aimed at type 2 diabetes mellitus (T2DM) patients, generally provides motivational support as well [15].
The literature recommends more research to study the impact of technical innovations on improved disease selfmanagement and medical outcome [17]. The prevention of diabetic complications requires good glycaemic control [16]. This study aimed to provide type 2 diabetes patients with remote active care and glycaemic control through the use of videophone technology without the need for them to attend hospital.
The aim of the study was to establish the effectiveness of the use of videophone technology in the glycaemic control of patients with diabetes.
Design and setting
This study was planned as a prospective, descriptive, randomized case control investigation. It was carried out in Ege University Faculty of Medicine, Endocrinology and Metabolism outpatient clinic. A total of 361 outpatients, whose ICD10 diagnosis codes were E10 or E14 and whose ICD9 codes were 250, were screened. The researcher telephoned a total of 361 patients, of whom 114 were found to be suitable for inclusion in the study. Using the systematic sampling method (using half ratio), 24 of these patients were chosen for the EG and another 24 for the CG. All agreed to participate in the study (24 was the number designated by Turkish Telekom who sponsored the study).
Systematic sampling is a statistical method involving the selection of elements from an ordered sampling frame. The most common form of systematic sampling is an equal-probability method. In this approach, progression through the list is treated circularly, with a return to the top once the end of the list is passed. The sampling starts by selecting an element from the list at random and then every kth element in the frame is selected, where k, the sampling interval (sometimes known as the skip):
K=N/n
Where n is the sample size, and N is the population size. Using this procedure each element in the population has a known and equal probability of selection. This makes systematic sampling functionally similar to simple random sampling. It is however, much more efficient (if variance within systematic sample is more than variance of population) .
The universe size N = 114 was divided by the sample size n = 24 (114/24 = 4.75), and was taken as about 5. A number from 1 to 5 was selected on a simple random number table. The number three was selected. Before the third file from the file 114 arranged in alphabetical order have been sampled. Then, one file from every five was included in the sample, and in this way 24 patients' files were selected. Patients in the CG received routine care, while the glycaemic control and consultations for patients in the EG were conducted using videophone technology.
Intervention
Control Group (CG)
Routine outpatient clinic monitoring methods were used for the patients in the CG. Patients were consulted at the endocrinology outpatient clinic at which they were being followed up. At face-to-face meetings, the patients' oral and written permission was obtained for participation in the study and use of the questionnaire form. After the third and sixth months, glycaemic control test results and daily blood glucose values were obtained at outpatient clinic consultations.In visits in the 3rd and 6th months, patients were given routine examinations in the diabetes clinic and insulin therapies were reviewed, after which necessary changes were made. Patients in CG were followed up by a hospital team (endocrinologist, dietician, diabetes nurse, etc.) CG support (risk and information management, use of resources etc.) and education on diabetes management were not provided to patients by researchers.
Experimental Group (EG)
The patients in the EG were also interviewed at the outpatient clinic and their consent for inclusion in the trial was obtained both orally and in writing. The videophone instrument was introduced to patients and they and their companions were shown how to use it; after checks were made at the outpatient clinic, videophone connections at patients' homes were established. Tele-monitoring by the researcher began in the first week after the videophone link had been installed in the patient's home. The information meeting began with the discussion of urgent topics (hyperglycaemia, hypoglycaemia, ketoacidosis, etc.) with the patient and his or her family. The conversations lasted 20 minutes on average.
The conversations were conducted and patients' A1c rates were monitored for medical glycaemic control at the first outpatient clinic visit. After that, videophone monitoring was performed once every week for 6 months. In the third and sixth months, face-to-face information meetings were organized. Patients' medical treatment and examinations were conducted by a hospital team (endocrinologist, dietician, diabetes nurse, etc). The patients were monitored by videophone for a total of 6 months by the researchers (telenursing). The researchers were contacted the patient by videophone every week. Information about the results of blood glucose monitoring and daily living problems (hypoglycemia, insulin administration, weight control, daily stresses, etc.) was given by the diabetes patients. Based on this information, education on diabetes management was provided in 20-minute interviews by videophone. If necessary, an endocrinologist, nutritionist, or other health worker directed, and researchers helped, the management of diabetes.
There is a difference between the glycaemic control levels of adults with T2DM who use videophone technology to receive frequent monitoring and those with diabetes mellitus who do not use videophone technology.
Statistical analysis
The SPSS (Statistical Package for Social Sciences (version 17, Chicago) was used for data analysis. Descriptive statistical methods (frequency, percentage, average, standard deviation) were used for the evaluation of the sociodemographic characteristics and the glycaemic control levels of the diabetes patients. The Repeated Measures Anova was utilised in the comparison of the HbA1c and blood glucose values recorded over the 6 month monitoring period. The results were bi-directionally evaluated within a 95% confidence interval and at a significance level of p<0.05.
Ethics
Patients who agreed to participate in the study received the informed consent forms one week before the baseline visit, and signed them before the randomisation. The study was carried out in accordance with the principles of the Helsinki Declaration and was approved by the Ethical Board of the Faculty of Nursing of Ege University (Document number 2009-51).
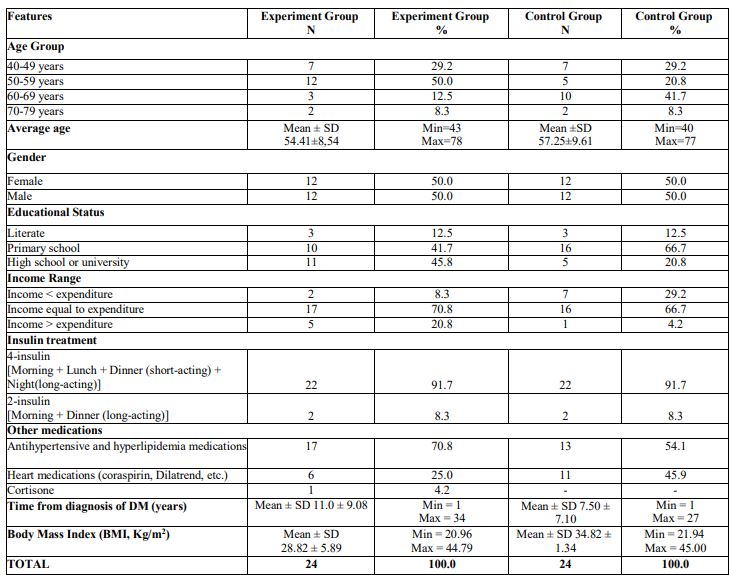
The mean age of the individuals in the EG was 54.41±8.54 years (Min=43 Max=78) and in the CG it was 57.25±9.61 (Min=40 Max=77). In both groups, 50% of the individuals were men and 50% women. In the EG, 41.7% had been educated up to primary school level and 45.8% up to high school or university level. In the CG 66.7% had been educated up to primary school level and 20.8% up to high school or university level. In the EG, 70.8% of patients, and in the CG 66.7%, had an income equal to their expenditure. The mean body mass index of the individuals in the EG was 28.82 ± 5.89 kg/m2 Min=20.96 Max=44.79) and in the CG it was 34.82±1.34 kg/m2 (Min=21.94 Max=45.00). In both groups, 91.7% of the individuals used insulin four times daily [Morning + Lunch + Dinner (short-acting) + Night(long-acting)]. In the EG 70.8% of patients and in the CG 54.1% used antihypertensive and hyperlipidemia medications.
Videophone monitoring was performed once every week for 6 months. It was shown that postprandial blood glucose levels of the patients in the EG (mean 163.48 ± 38.64 mg/dl) were higher than preprandial blood glucose levels (mean 159.48 ± 40.71 mg/dl) at 6 months. It was determined that preprandial (mean 173.03 ± 65.07 mg/dl ) and postprandial (mean 175.88 ± 66.69 mg/dl) blood glucose levels of the patients in the CG were very close to each other at 6 months. When the two groups were compared, it was was found that the morning fast blood glucose levels of patients in the EG (mean 159.48 ± 40.71mg/dl) were lower by 13.55 ± 52.89 mg / dl than the morning fast blood glucose levels of the diabetic patients in the CG (mean 173.03 ± 65.07 mg/dl) at 6 months. It was determined that the morning post prandial blood glucose levels of patients in the EG (163.48 ± 38.64mg/dl) were lower by 12.40 ± 52.66 mg / dl than the morning post prandial blood glucose levels of the diabetic patients in the CG (mean 175.88 ± 66.69 mg/dl) at 6 months. Noon post prandial blood glucose levels of patients in the EG (155.56 ± 39.86 mg/dl) were lower by 20.32 ± 51.20 mg / dl than noon post prandial blood glucose levels of the diabetic patients in the CG (mean 174.38 ± 62.55mg/dl) at 6 months. Finally, evening post prandial blood glucose levels of patients in the EG (162.55 ± 41.29 mg/dl) were lower by 14.29 ± 53.49 mg / dl than evening post prandial blood glucose levels of the diabetic patients in the CG (mean 176.84 ± 64.70mg/dl) at 6 months. However, there was no statistically significant difference in blood glucose levels between the groups (p>0.05) (Table 2).

It was found that patients in the EG and CG showed a homogenous distribution in terms of mean age and gender distribution. In developed countries diabetes is an illness seen among people over 64 years old, but it is seen more often in people between the ages of 45 to 64 years in developing countries . In Turkey, at least 10% of people aged 40 and above are reported to have diabetes [4]. T2DM is most common among those in the over-60 age group and is more widespread among men than among women [13]. Age, a non-genetic factor, affects the incidence of the illness. The rate of type 2 diabetes in Turkey is 17.2% among women and 16% among men [4].
In a study by Buyssea et al., 30.9 % of patients participating in the study were high school and university graduates . In a study by Kartal et al., it was reported that 19.1% of the patients taking part in the research were high school graduates and 9.1% were university graduates . In our study, 41.7% of patients in the EG were educated up to primary school level and 45.8% up to high school or university level. Also, 66.7% in the CG were educated up to primary school level and 20.8% up to high school or university level.
It was was found that at 6 months the morning fast blood glucose levels of the patients in the EG were lower by 13.55 ± 52.89 mg / dl than those of the patients in the CG. In a cohort study by Arsand et al., who looked at mobile phone-based self-management tools for type 2 diabetes, it was determined that the blood glucose levels of diabetic patients being tele-monitored by doctors and nurses over six months fell from160 mg/dl to 140 mg/dl. This was statistically significant (No p value of in this study).
It was determined that the A1c levels of the individuals in the EG were significinatly lower by 0.49% in total at the end of the six-month monitoring and that the A1c levels of the individuals in the CG were higher by 0.17 % in total at the end of the six-month monitoring. The A1c values of 23.2% of the individuals participating in the TURDEP study were found to be in the high risk range . The study shows similaries to the prevalence study in Turkey. This conclusion supports the hypothesis: "there is a difference between the glycaemic control levels of diabetic individuals frequently monitored by videophone technology and those who were not monitored by videophone technology or trained face to face.
In a randomized controlled tele-monitoring study by Stone et al. (2010), it was found that the A1c levels of diabetic individuals in a tele-monitoring group were lower by 1.7 – 0.8 % in the third and sixth months compared with a telephone group (P < 0.001) . In a tele medicine cohort study on type 2 diabetics by Kesavadev et al. (2012), it was determined that the mean±SD A1c value was 8.5±1.4% at the initial visit and was reduced to 6.3±0.6% at 6 months (P<0.0001) . In our study similar to these studies, decreased A1c levels were found at sixth months.
In the ELENOR study (2011), tele-care and self blood glucose monitoring groups were compared in type 2 diabetics. The A1c levels of patients who used tele-care fell from 8.8% to 7% at the end of the 32nd week and the A1c levels of patients in the self blood glucose monitoring group fell from 8.9 % to 7.5 % at the end of the 32nd week. It was shown that the A1c levels of the tele-care group were reduced by 1.8 % and the A1c levels of the other group were reduced by 1.4% (P < 0.001) . In a tele-medicine study on type 2 diabetics by Narayanan et al. (2012), the A1c levels of diabetic patients were 9% higher than at first. It was found that the A1c levels of diabetic patients were 0.03% lower at the end of the third year, 0.28% lower at the end of the second year and 0.56% lower at the end of the first year . The authors failed to find a significant difference in HbA1c between the two groups. Similarly, these studies showed an improvement in glycaemic control using tele-medicine.
In a meta-analysis examining the effect on diabetes management by mobile phones by Liang et al. (2010), data from twenty-two studies performed between 2004 and 2010 were investigated. Ten studies were performed to monitor the six month average of A1c levels with type 2 diabetics . In subgroup analysis, 11 studies of Type 2 diabetes patients reported significantly greater reduction in HbA1c than studies of Type 1 diabetes patients (0.8 - 0.3%; P = 0.02). In a meta-analysis, randomized controlled studies found that the A1c levels of patients were 0.2 – 0.8 % lower than other studies with non-randomized designs. In initiatives (most trials used a mobile phone short message service (SMS) to deliver blood glucose test results and selfmanagement information) it wass established that the daily, weekly and monthly A1c levels of patients were reduced by 0.6% by mobile phone intervention. The meta-analysis study showed that tele-medicine intervention methods for diabetes care led to statistically significant improvements in glycaemic control and self management .
Tele-monitoring is an increasingly used treatment approach to chronic diseases. The approach reinforces the collection and interpretation of disease symptoms and findings, and attempts at disease prevention. In recent times the application of modern technologies such as e-health, tele-care and tele-medicine has been targeted at the treatment of diabetes patients. The increase in the use of technology in diabetes treatment allows improved communication between nurses and patients, the collection of reliable information, and the provision of a comfortable life to patients. Yes, my comments. So, I took out resource numbers.
The needs of patients with different metabolic control needs are met through the use of technical instruments such as videophones.
When the two groups in the study were compared, it was was found that the A1c and blood glucose levels of the diabetic patients in the EG were lower of than those of the individuals in the CG. This showed that videophone technology can be useful in the glycaemic control of diabetic patients in Turkey.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
